A 50 YEAR OLD PATIENT WITH CERVICAL MYELOPATHY
May 21,2021
Amisha Jaiswal,MBBS 8th semester
Roll no:03
This is online E-log book to discuss our patient’s de-identified Health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s Problems through series of inputs from available global online community of experts with an aim to solve those patient’s clinical problems with collective current best evidence-based inputs. This is the E-log book also reflects my patient centred online learning portfolio and your valuable inputs on comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of" patient clinical data analysis” to develop my competency in reading and comprehending clinical data Including history,clinical findings ,investigations and come up with diagnosis and treatment plan.
A 50 YEAR OLD MALE WITH CERVICAL MYELOPATHY
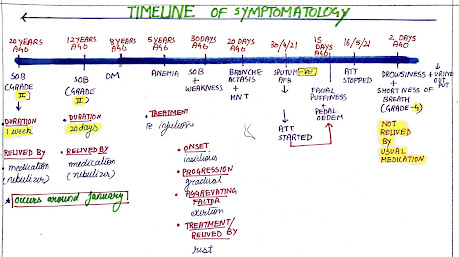
Following is the view of my case(history as per date of admission)
CASE:
50-year-old male patient presented to hospital with complaints of weakness of all four limbs since 8 PM yesterday.
HISTORY OF PRESENTING ILLNESS:
-Patient was apparently a symptomatic before 8 PM yesterday then he developed weakness of all four limbs which was sudden in onset and preceded by history of Alcohol binge and fall.
-No H/o slurring of speech
-No H/o fever
HISTORY OF PAST ILLNESS:
-History of hypertension since five years, patient is on regular medication
-No H/o of loss of consciousness
-No H/o of DM,Epilepsy,TB
-No similar complaints in past
-No H/o past surgery
PERSONAL HISTORY:
Diet- mixed
Appetite-normal
Sleep-adequate
Bowel and bladder movements-regular
Addictions-drinks occasionally(90 ml everyday)
FAMILY HISTORY
no history of DM,HNT,heart diseases,stroke
GENERAL EXAMINATION:
The patient was conscious,coherent and cooperative and well oriented to time place and person.He is sitting comfortably on the bed ,moderately build and well nourished.
Pallor-absent
Icterus-absent
Clubbing-absent
Cyanosis-absent
Lymphadenopathy-absent
Edema - absent
VITALS-
Temperature -98.6^C
Pulse rate-72/min
Respiratory rate-18/min
BP-140/90mm of Hg
GRBS-131mg%
SYSTEMIC EXAMINATIONS:
CVS-S1 and S2 heard,no added mummers and thrills heard
ECG

RESPIRATORY SYSTEM-normal vesicular breath sounds heard
ABDOMEN-soft and non tender,no organomegaly
CNS
- no sensory symptoms are present
-motor system examination
LEFT RIGHT
POWER
upper limb 1/5 1/5
Lower limb 0/5 0/5
REFLEXES
biceps Absent Absent
Triceps Absent Absent
Knee Absent Absent
Ankle Absent Absent
CRANIAL NERVES- normal
GLASGOW SCALE-15/15
INVESTIGATIONS
HAEMOGRAM
-PCV: 38.9(decreased )
-RBC count: 4.25(decreased)
-SMEAR :normocytic normochromic

COMPLETE BLOOD PICTURE

LIVER FUNCTION TEST
-alkaline phosphate : 167IU/L(increased)
-total proteins : 6.2gm/dl (decreased)

SMEAR URIC ACID

BLOOD UREA

SMEAR CHLORIDE

APTT

PROTHROMBIN TIME

CK




PROVISIONAL DIAGNOSIS
-C3-C6 OPLL that is osteomalacial changes referred for neurosurgical intervention
-quadriparesis
-hypokalemia
TREATMENT
- INJ.OPTINEURON 1AMP IN 100 ML NS IV/OD
-IN THIAMINE 1 AMP IN 100 NS/IV/TID
-TAB DEXAMETHASONE 8MG BD
-GBRS CHARTING 6TH HOURLY 4.TAB.DOLO 650 MG/PO/TID
- Ortho referal and referred to higher center as per orthopaedicians advice.
ADVICE AT DISCHARGE
-Patient being referred to higher Centre I/V/O NEUROSURGICAL INTERVENTION
-SURGERY ADVISED: C3-C6 screw fixation,C3-C6 lamenectomy
QUESTIONS
-What is myelopathy hand ?
-What is finger escape ?
-What is Hoffman’s reflex?
*Under the guidance of Dr. Saicharan and Dr.Vilasith(intern)
Comments
Post a Comment